


Why I'm cautious about taking any drugs or peptides regularly

Overall there have been hype cycles about some drugs or peptides causing a lot of benefits for people. Fit 45-year-old cardiologists with CAC scores of 0 and good blood work take statins prophylactically. Metformin and rapamycin were and are still hyped by many people as potential longevity medications, even if their bloodwork showed no insulin resistance or other metabolic issues beforehand.
Later, you often learn about the potential downside of taking these meds.
Statins
Statins can make gaining muscle more difficult, cause muscle weakness, further progress sarcopenia, and cause cognitive issues and other hormone synthesis issues since cholesterol is also the basis for creating hormones in the body. There are many more details that others have dived into, to the point where taking not statins unless absolutely necessary has become a trend on biohacker social media.
I had a worried-well friend wanting to take a statin at 40 because he was worried about developing CVD issues later in life; I had to caution him against it due to all of these downsides he was unaware of and told him to research it more if he was healthy currently.
Metformin
Metformin has its issues. It may improve your blood sugar numbers, but it also similarly reduces muscle mass by reducing exercise performance. It can introduce GI issues, add stress to your kidneys, cause B12 absorption issues, interfere with mitochondrial function, and more. Depending on your current state, the 'improvement' might be worse than the disease.
Rapamycin
Rapamycin is an anti-organ rejection drug that became popular due to its associated effects of reducing mTOR, inflammation, and other issues. However, being an immunosuppressant can cause issues that come with that entire category of medications. It can also make your metabolic health worse by inducing insulin resistance and increasing triglycerides, along with inducing fertility issues.
Goodhart's Law-ing ourselves to death
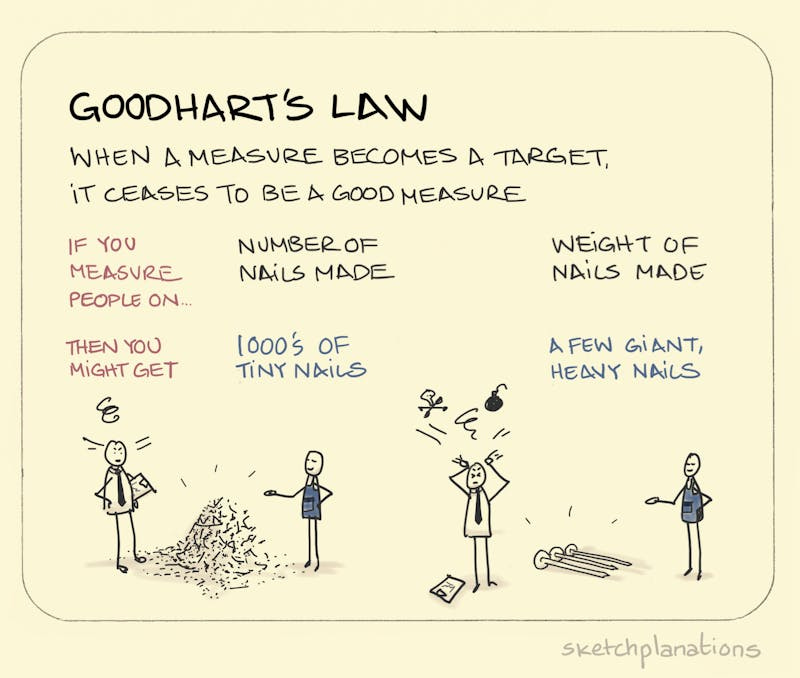
“Goodhart's law is the idea that when a metric is used as a target, it becomes less effective at measuring what it's intended to measure. This is because people are incentivized to manipulate the metric to receive a reward.”
Humanity is very prone to oversimplifying things and pursuing optimizing easy numbers. Understanding a more complex, nuanced system is often too much, so we try to over-optimize singular numbers that are easier to understand. This can often lead us to harm ourselves rather than improve our situations. I believe potentially many of the above things are us goodharting ourselves in the wrong direction.
Cholesterol and Polyunsaturated Fats
Similarly, Ancel Keys in the 1950s led the cholesterol revolution in heart disease, which led to entire generations of doctors and patients believing that total cholesterol is the only thing that matters. Follow-up research showed that saturated fat increased cholesterol numbers, which led to a general war on saturated fat ever since then and the widespread adoption of polyunsaturated vegetable/seed oils. This belief became so widespread and popular that activist millionaires self-funded campaigns to change restaurants to use vegetable oils over saturated fats for their recipes. This led to the (in)famous change of McDonald’s making their fries with beef tallow to vegetable oils.
Now, slowly, as more and more research shows, it’s not just the cholesterol but the details of the entire system that matter more. Basic things like your HDL to LDL ratio are now finally standard practice. The size of the particles matter, and other things such as Apo-B or Apo-A also matter. But to this day, not even cholesterol particle fractionation or measuring Apo-B or A is part of a standard annual checkup. The vast majority of people don’t even know about these biomarkers.
On top of all this, cholesterol is probably just a secondary indicator of cardiovascular disease. High cholesterol numbers and the large amount of cholesterol inside plaque formation occur because it is a repair response to inflammation and other arterial wall damage, and (epi)genetically, some people have a stronger response than others, showing the variation in populations.
Reducing cholesterol is like getting rid of firefighters; saying that is now an indication of fewer fires in a city because you cannot see the fire. We have probably goodharted ourselves in completely the wrong direction, and other inflammation and metabolic indicators should be the targeted intervention and measurements, not directly reducing cholesterol unless the patient is close to closing off their arteries or generating blood clots as an emergency measure. This idea alone is very controversial because medicine is slow to adopt newer research.
To add more irony, research is also starting to show that large amounts of polyunsaturated fats in a diet can cause more metabolic dysfunction, which leads to more cardiovascular issues. The society-wide push to move away from saturated fat could’ve been a key factor in why cardiovascular disease has gotten worse over the years.
mTOR
Reducing mTOR is a current longevity trend, but 20 years from now, we might discover some nuance that makes this idea that we thought was good, is a bad idea, as cholesterol and heart disease have shown above. Even mTOR reduction itself is controversial today. People in one camp say reducing mTOR causes worse issues via muscle loss and long-term muscle retention, which are important for longevity. At the same time, other research points out the benefits of reducing overall cell growth. Some people want to reduce mTOR significantly since they think you’ll live the longest with it at a low state, while others say having it more balanced is the better idea, especially since you’ll keep more muscle mass that way. Overall, the focus on reducing mTOR alone smells a lot like a Goodhart oversimplification.
Conclusion
Because of all of the above and a bunch of other things I didn’t get into for brevity, I am cautious about adopting any new medication unless it is necessary. If I am considering it, then I would want to research it for a while before adding it to my repertoire. I would suggest doing the same for yourself, especially for things that you might use for a long time. Usually, I try to solve my issues or improve my goals with dietary, exercise, or lifestyle interventions first and then consider medications if those things are not working as well as I would like.
100%. "Just in case" is a terrible strategy in complex systems. Would you pour random chemicals into your car's gas tank "just in case" they help? No! Your body is way more complicated than that.